- Research
- Open access
- Published:
Development and evaluation of 3D-printed tumor palpation models for surgical training and patient education
3D Printing in Medicine volume 10, Article number: 41 (2024)
Abstract
Breast cancer screening is implemented as part of governmental healthcare policy in many countries. While breast imaging tests contribute to reducing mortality, some breast cancers may emerge between these screenings. Consequently, it is crucial for women to be vigilant about any changes in their breasts to facilitate the early detection of breast cancer. Recently, the application of 3-dimensional printing technology in the medical field has expanded, including uses in medical imaging and surgical training. In this study, we developed 3D-printed palpation models for breast tumor detection and surveyed seven surgeons specializing in breast care to evaluate the usability of the models. As a result of the survey, we created a model that obtained a maximum mean rating of 7.1(maximum rating 10, minimum rating 3) on the item 'How accurately does the model simulate the feel of a real tumor?' on a scale from 1 to 10. Although there is some variation in the average value, through this study, we found that it is possible to create a model that is quite close to the actual tumor depending on the materials and shape of the models. Our findings demonstrated the potential use of personalized models both in medical trainee and patient education.
Background
Breast cancer is the most common cancer among females worldwide, exerting a considerable medical, social, and economic impacts [1, 2]. Previous studies have demonstrated that screening mammography significantly contributes to reducing breast cancer mortality [3], leading to its adoption as a governmental healthcare policy in Japan. The current breast cancer screening policy in Japan recommends mammography every two years for women aged 40 and above. However, despite these measures, some breast cancers are detected between scheduled screening examinations, known as interval breast cancers [4], highlighting the limitations of current screening programs. For this reason, it is vital for individuals to regularly monitor changes in their breasts, fostering breast awareness, to aid in the early detection of breast cancer. This approach complements screening programs by addressing gaps in detection and emphasizing the importance of personal vigilance in breast health maintenance [5].
Educating the public on breast health is essential for raising breast awareness, with silicone breast palpation simulators and models frequently employed towards this end [6]. Furthermore, numerous studies have underscored the effectiveness of breast palpation models in medical student education [7, 8]. Recent studies have demonstrated the efficacy of 3D-printed models for medical training purposes across various specialties. For instance, Kiesel et al. (2022) developed a 3D-printed model of the female pelvis for hands-on training of gynecological examination, which showed significant improvement in students’ satisfaction and knowledge gain [9]. Similarly, Bertolini et al. (2024) reported on the effectiveness of a 3D-printed simulator for transcatheter edge-to-edge repair of the tricuspid valve, highlighting its potential in enhancing medical training for complex procedures [10]. However, the high cost of these models precludes their widespread distribution to patients. Additionally, the uniformity of existing models fails to accurately reflect the diverse characteristics and masses found in different individuals’ breasts.
Recent advancements in 3-dimensional printing technology have broadened its application within the medical field, encompassing areas such as medical imaging and surgical training. For example, Sheha (2019) et al. [11] detailed their use of a 3D printer to fabricate models from CT images of a patient’s spine before sarcoma surgery, aiding in understanding the lesion’s anatomy and facilitating preoperative planning. Hanisch (2020) et al. [12] used models created by a 3D printer based on actual patient data, for surgical training of dental students, and found them to be as just as good as conventional typodont models. The study also pointed out that the use of a 3D printer provides more realistic surgical training.
Building on these findings, we developed 3D-printed palpation models of breast tumors and surveyed surgeons specializing in breast care to assess the models’ utility. This study presents the survey findings, discusses the recommended modeling methods based on surgeons’ feedback, and explores the models’ potential benefits for medical and patient education.
Methods
Development of breast tumor palpation models using 3-dimensional printing technology
Initially, 3D geometry data, with a 15 mm diameter sphere, embedded at the bottom of a 20 mm cube, was generated using 3D-CAD software, ZW3D2023 (ZWSOFT CO., LTD.) (Fig. 1). The inside of the sphere was filled with support material AR-S1(KEYENCE CORPORATION). We used the AGILISTA-3200 (KEYENCE CORPORATION) for 3D printing, which employs Material Jetting technology. This printer offers high-resolution capabilities (minimum layer thickness of 15 μm) and the ability to print with multiple materials simultaneously, allowing us to create models with varying properties in a single print job. On the other hand, the cube was printed using AR-G1L (KEYENCE CORPORATION) and its wall thicknesses were varied to be 0.5 mm, 1.0 mm, and 1.5 mm, resulting in three distinct models designated as Models A, B, and C, respectively. The interiors defined by these walls were filled either with support material (Fig. 2). In addition, the 3D geometry data of a similar cube with one face removed was generated using the same methodology, and models were created with the thickness of the cube walls varied to 0.5 mm, 1.0 mm, and 1.5 mm, with the interior filled with urethane gel, designated as Models D, E, and F (Fig. 3). As a result, we generated a total of six models based on the combinations of three wall thicknesses and two types of fillers (Fig. 4). The urethane gel used was “Human skin gel (Hardness 0)” (EXSEAL CO, LTD.).

An overall view of the 3D data and the variability in “t.”

The cube’s central cross-section and the support material filling (“※”)

The cube’s central cross-section and the urethane gel filling (“*”)

A completed model example (Fig. 2A, 0.5 mm thickness and support material filling)
Questionnaire survey
To evaluate the models, a questionnaire comprising the following four items was developed.
-
Q1. How accurately does the model simulate the feel of a real tumor? (1 = not at all, 10 = about the same as the real one)
-
Q2. How would you rate the tumor’s firmness? (1 = too soft, 5 = just right, 10 = too hard)
-
Q3. How would you rate the firmness of the tissue surrounding the tumor? (1 = too soft, 5 = just right, 10 = too hard)
-
Q4. An additional section was provided for comments.
Participants were required to rate questions Q1 to Q3 on a scale from 1 to 10. If the model’s wall thickness prevented their fingers from reaching the tumor, making evaluation difficult, they were instructed to mark their response as “N/A.” Question 4 allowed for free comments. Palpation was conducted either with the index finger alone or by applying pressure with both the thumb and index finger. The responses to the questionnaire were analyzed using a Mann-Whitney U test, with specific comparisons made between different support materials and wall thicknesses to evaluate how accurately the models simulate real tumor characteristics. All statistical analyses were performed using R version 4.1.2. P-values less than 0.05 were considered to indicate statistical significance.
Results
Seven surgeons, all specializing in breast care, were invited to palpate each model, followed by participation in a questionnaire survey. The cohort of surgeons comprised two with over 30 years of clinical experience, one with over 20 years, three with more than 10 years, and one with less than 10 years of experience. The questionnaire data were collected and analyzed, yielding the following findings. Regarding Q4, which was intended for free-text responses, we did not receive any comments from the participants.
Analysis of support material models
In Q1, palpation models garnered mean scores of 5.9, 6.0, and 3.7 for Models A, B, and C respectively, with median scores of 7.0, 5.5, and 4.0. The highest scores were 8 for Models A and B, and 5 for Model C, while the lowest scores were 2 for Models A and C, and 5 for Model B. Model B received one N/A response for Q1 and two for Q2, and Model C had six N/A responses for Q2 and two for Q3, with Model A having no N/A responses. The Mann-Whitney U test, detailed in Fig. 5B, evaluated the questionnaire responses for each model, indicating no statistical significance between Models A and B (Q1 p=0.8988), a possible trend towards significance between Models A and C (Q1 p=0.0540), and a statistically significant difference between Models B and C (Q1 p=0.0052). For Q3, statistically significant differences were found between Models A and B (p=0.0048) and A and C (p=0.0108), but not between Models B and C (p=0.6578). Due to the N/A responses, Q2 was not applicable for statistical comparison between Models A and B or B and C.

A Results of the questionnaire on models using support material. B Comparison by Mann-Whitney U tests of each questionnaire item on models using support material
Analysis of urethane gel models
Following the assessment of support material models, the analysis of urethane gel models was conducted as depicted in Fig. 6A. In Q1, models D, E, and F achieved average values of 7.1, 3.6, and 5.9 respectively, with median values corresponding to 7.0, 3.0, and 7.0. The maximum ratings given were 10 for Model D, 7 for Model E, and 3 for Model F, with the minimum ratings being 3, 2, and 1 for each respective model. Each model had one instance where Q2 was marked as N/A by a participant. Mann-Whitney U tests were performed to compare responses for each model, with the results displayed in Fig. 6B. The analysis revealed a statistical significant difference between Models D and E for Q1 (p = 0.0077), but no statistical significant difference was observed between Models D and F (p = 0.3572) or E and F (p = 0.0680) for the same question. For Q3, the results indicated a marginal trend towards significance between Models E and F (p = 0.0520), while the other comparisons showed no statistically significant differences. As with the support material models, Q2 comparisons were not applicable due to N/A responses. These results complement the earlier findings from the support material model analysis, providing further insights into the palpation models’ effectiveness using urethane gel.

A Results of questionnaire on models using urethan gel. B Comparison by Mann-Whitney U tests of each questionnaire item on models using urethan gel
Discussion
The evaluation of palpation models by seven experienced breast care surgeons revealed discernible differences in the perception of model fidelity based on material and design in this study. The analysis showed that models constructed with urethane gel generally received higher mean and median scores compared to those using support material, with Model D attaining the highest mean score of 7.1. Notably, the wall thickness appeared to be a critical factor in the realism of the models; thinner walls tended to be associated with higher ratings of similarity to actual tumors. However, there was a trade-off between thinness and durability, underscoring the need for careful optimization of wall thickness. These findings are crucial as we consider the practical application and potential benefits of these models in medical training and patient education.
-
1.
Optimal modeling method
Whether the model was filled with support material or urethane gel, models with thinner walls received higher ratings. However, excessively thin walls may compromise the model’s integrity during palpation, posing a risk of breakage. Therefore, it is essential to calibrate wall thickness to balance durability with a realistic palpation experience. When comparing fillers (as shown in Fig. 7), models with urethane gel generally achieved higher maximum and average scores than those with support material, indicating the superior tactile quality of urethane gel. Notably, one respondent rated the Model D as ‘10’, equating it nearly to the real-life palpation experience, suggesting the successful replication of a practical model.
Fig. 7 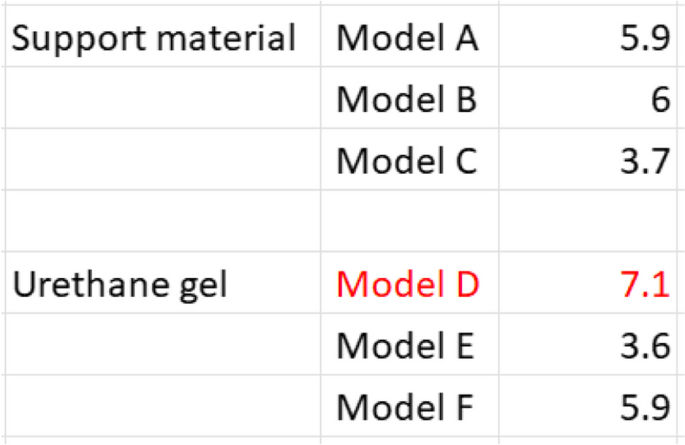
Average scores of Q1 by filler material
Nevertheless, this study's limitation lies in the model's cubic shape and 20mm size, which does not emulate the actual breast and cannot be effectively evaluated using palm palpation. Additionally, as all participants were experts in breast care, further analysis by medical students and doctors who are not specialized in breast cancer will be needed.
-
2.
Usefulness of 3D printed palpation models in medical education and patient education
The developed model has potential as an effective training tool for medical students and residents learning breast palpation. Evidence from Pilgrim et al. [7] suggests that hands-on practice with a silicone breast model, coupled with immediate feedback on a female volunteer, is more beneficial than theoretical lectures alone. Similarly, Schubart et al. [8] have found breast palpation simulators to be particularly valuable for medical students with limited clinical experience. Although the advantages of palpation models in medical education are well-established, such models are generally costly and standardized. Our model promises to be cost-effective for educational purposes, with the added advantage of customizable shapes and sizes via computer adjustments, enabling the creation of diverse breast tumor models.
Further, distributing 3D-printed models like those in this study to the general public could potentially advance breast cancer detection. Research by Idrees et al. [13] has demonstrated the effectiveness of breast palpation models for teaching self-examination in India, thereby enhancing breast awareness. In clinical settings, masses that cannot be immediately classified as malignant are often monitored over time. The capability of 3D printing technology to produce highly individualized models for each patient's mass could lead to more personalized consultation guidelines.
-
3.
Future directions
This study lays the groundwork for several promising research avenues. First, we plan to develop a wider range of models with varying tumor sizes, depths, and textures to more comprehensively simulate the diversity of breast tumors encountered in clinical practice. Second, we aim to conduct a larger-scale evaluation involving not only experienced surgeons but also medical students and residents to assess the models' effectiveness in different stages of medical education. Additionally, we intend to explore the integration of these 3D-printed models with virtual reality (VR) technology, potentially creating a hybrid learning environment that combines tactile feedback with visual guidance. Finally, we will investigate the possibility of customizing models based on individual patient data, which could revolutionize preoperative planning and patient education in breast cancer care.

Conclusion
Our investigation into the production methods of 3D-printed tumor models has demonstrated a clear preference among surgeons for models crafted with urethane gel over those with support material, particularly when the models feature thinner walls. These results highlighted the implication of urethane gel in creating high-fidelity models. Development of new filling materials and optimization of shape will provide more effective models and contribute to medical education as well as the early detection of breast cancer.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request. Summary statistics and aggregated data are included in this published article and its supplementary information files.
Data availability
Date availability: We share our date in a supplement file.
References
Iima M, Le Bihan D. The road to breast cancer screening with diffusion MRI. Front Oncol. 2023;13:993540.
Hattori M, Novick D, Takaura K, Tanizawa Y, Kawaguchi T, Haro JM, Monistrol-Mula A, Onishi A, Iwata H. A systematic literature review of prognostic factors in patients with HR+/HER2- advanced breast cancer in Japan. Jpn J Clin Oncol. 2021;51(10):1498–508.
Ohnuki K, Tohno E, Tsunoda H, Uematsu T, Nakajima Y. Overall assessment system of combined mammography and ultrasound for breast cancer screening in Japan. Breast Cancer. 2021;28(2):254–62.
Grassmann F, He W, Eriksson M, Gabrielson M, Hall P, Czene K. Interval breast cancer is associated with other types of tumors. Nat Commun. 2019;10(1):4648.
Uematsu Takayoshi Y, Kasahara A, Suzuki H, Takahashi. Hiroko Tsunoda Breast Awareness Assoc. Breast Cancer Screen. 2020;29(1):27–33.
Akhtari-Zavare M, Juni MH, Said SM, Ismail IZ, Latiff LA, Ataollahi Eshkoor S. Result of randomized control trial to increase breast health awareness among young females in Malaysia. BMC Public Health. 2016;16:738.
Pilgrim C, Lannon C, Harris RP, Cogburn W, Fletcher SW. Improving clinical breast examination training in a medical school: a randomized controlled trial. J Gen Intern Med. 1993;8(12):685–8.
Schubart JR, Erdahl L, Smith JS Jr, Purichia H, Kauffman GL, Kass RB. Use of breast simulators compared with standardized patients in teaching the clinical breast examination to medical students. J Surg Educ. 2012;69(3):416–22.
Kiesel M, Beyers I, Kalisz A, Wöckel A, Quenzer A, Schlaiß T, et al. Evaluating the value of a 3D printed model for hands-on training of gynecological pelvic examination. 3D Print Med. 2022;8:20.
Bertolini M, Carlini L, Clementini L, Dall’Aglio M, Colombo G, Capelli C. 3D printed training simulator for transcatheter edge-to-edge repair of the tricuspid valve: a proof-of-concept. Annals 3D Print Med. 2024;15:100157.
Sheha ED, Gandhi SD, Colman MW. 3D printing in spine surgery. Ann Transl Med. 2019;7(Suppl 5):S164.
Hanisch M, Kroeger E, Dekiff M, Timme M, Kleinheinz J, Dirksen D. 3D-printed surgical training model based on real patient situations for dental education. Int J Environ Res Public Health. 2020;17(8):2901.
Idrees S, Mayilvaganan S, Jagannath S, Mishra P, Chand G, Mishra A, Agarwal G, Agarwal A. Validation of cost-effective model for breast self-examination. Ann Med Surg (Lond). 2023;85(2):166–71.
Acknowledgements
We extend our sincere gratitude to the seven surgeons from the Department of Surgery at the Jikei University School of Medicine who participated in our survey. Their expertise and invaluable feedback were essential in evaluating our 3D-printed palpation models, significantly enhancing this study.
Funding
This study is partly supported by the Taiju Life Social Welfare Foundation’s 56th Medical Grant. There was no other funding.
Author information
Authors and Affiliations
Contributions
H.K. prepared the manuscript, created the 3D-printed palpation models, collected and analyzed the survey data. A.F. oversaw the entire study, designed the research, and interpreted the results. S.F. provided guidance on 3D printing technology and contributed to the study design. R.M., M.K., and H.N. reviewed the manuscript content. H.N. also supervised the entire study. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Katori, H., Fushimi, A., Fujimura, S. et al. Development and evaluation of 3D-printed tumor palpation models for surgical training and patient education. 3D Print Med 10, 41 (2024). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s41205-024-00234-x
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s41205-024-00234-x